

Introduction
The monitoring of a patient's response to chemotherapy, called, measurable residual disease (MRD) is one of the most important predictors of outcome in Acute Myeloid Leukemia (AML). Although universally applicable, FCM-MRD for AML suffers from low sensitivity as compared to precursor B lineage acute lymphoblastic leukemia. Here, we evaluated the clinical utility of error corrected next generation sequencing (NGS) to detect MRD (NGS-MRD) in AML using single molecule molecular inversion probes (smMIPS). We compare NGS-MRD and FCM-MRD and determine their impact on patient outcome. We demonstrate that error corrected NGS-MRD at early timepoints in therapy is an independent and significant predictor of outcome in patients of AML treated with conventional therapies.
Methods
We created a 35 gene "hotspot" panel comprising of a pool of 302 smMIPS. In brief, this panel covers regions of 35 commonly mutated genes in AML.FLT3-ITD were detected using a novel one-step PCR based NGS assay. Post mapping, singleton reads (originating from one UMI) were discarded and consensus family based variant calling was performed. We then created a site and mutation specific error model to ascertain the relevance of an observed variant at each site. A limit of detection (LOD) experiment demonstrated a lower detection limit of 0.05%. For FLT3-ITD the LOD was 0.002%. A total of 393 adult patients of AMLwere accrued over a period of six years.Patients were treated with standard 3+7 induction followed by 3 doses of HiDAC. Allogeneic bone marrow transplantation was offered where feasible. Somatic mutations at diagnosis were evaluated using a smMIPS based 50 gene myeloid panel which was applicable to 327 patients [83.2% of AMLs, median 2 mutations per case (range 1 - 6 trackable mutations)].MRD assessment could be performed in 201 adult patients of AML in morphological remission (not performed in the rest because of suboptimal quality DNA at MRD time points or missing sample).Samples were sequenced on multiple S4 flow cells of a NovaSeq 6000 using 150PE chemistry.FCM-MRD was obtained from the bone marrow at end of induction (PI, n=200) and end of first consolidation cycle (PC, n=98). NGS-MRD sample also obtained at the same time points (PI, n=196& PC, n=127) from the bone marrow (n=266) or peripheral blood (n=45).
Results
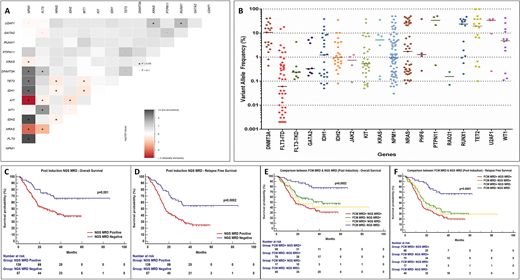
The interaction of mutations that were trackable at diagnosis can be seen in Figure 1A. A total of 345 mutations could be detected in 196 patients (Figure 1B) with a median VAF of 1.01% [0.82% after exclusion of mutations in DNMT3A, TET2, ASXL1 (DTA) genes; (median of 2 mutations for PI and one for PC timepoint)]. The median consensus read coverage was 11,127 for the smMIPS assay, whereas for the FLT3-ITD assay it was 13,96,366.The median follow-up of the cohort was 42.3 months. The presence of NGS-MRD (70.9%) was associated with inferior overall survival (OS; p=0.001) [hazard ratio(HR)- 2.24; 95% confidence interval (CI)- 1.47 to 3.43] and relapse free survival (RFS; p=0.0002) [HR- 2.28; 95% CI- 1.58 to 3.31] at PI time point as well as PC time points [40.94% positive; OS (p=0.008)(HR- 1.92; 95% CI- 1.14 to 3.22) and RFS (p=0.004)(HR- 1.90; 95% CI- 1.18 to 3.05)].Similarly, FCM-MRD (44%) was predictive of inferior OS (p=0.0002)(HR- 2.08; 95% CI- 1.38 to 3.13)and RFS (p=0.0008)(HR- 1.81; 95% CI- 1.26 to 2.60) at PI as well as PC time points [21.4% positive, OS (p=0.04)(HR- 1.87; 95% CI- 0.89 to 3.91) and RFS (p=0.001)(HR- 2.38; 95% CI- 1.17 to 4.81)].
On multivariate analysis post induction NGS MRD emerged as the most important independent prognostic factor predictive of inferior outcome for OS [HR- 1.94; 95% CI-1.15 to 3.27; (p<0.0001)]as well asRFS[HR-2.05; 95% CI-1.30 to 3.23; (p<0.0001)].On incorporating results combining both the MRD modalities,patients that were positive by both techniqueshad a significantly inferior outcome with respect to OS (p=0.0002; HR- 4.66; 95% CI- 2.71 to 8.0)and RFS (p=0.0001; HR- 4.03; 95% CI- 2.51 to 6.47) at PI timepoint as well as PC timepoint [OS (p=0.02; HR- 3.73; 95% CI- 1.07 to 12.97) and RFS (p=0.0015; HR- 4.17; 95% CI- 1.27 to 13.7)] as compared to patients negative by both modalities (Figure 1E,F)
Conclusion
In conclusion, we demonstrate that error corrected panel-based sequencing is feasible for MRD monitoring in AML and may offer an advantage over existing techniques. Maximum clinical utility may be leveraged by combining FCM and NGS modalities.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal